In 2018, Eswatini's laboratory system was experiencing challenges in meeting the need for viral load (VL) testing for people living with HIV. Viral load testing coverage was only 55 percent nationally, which meant that many patients being treated for HIV could not access testing to know their health status, and their clinicians could not monitor their treatment results.
At this time, Eswatini was just beginning to conduct viral load testing for HIV, having introduced a few VL instruments into its laboratory system. Viral load testing had become the preferred method of testing for HIV; the previous primary method, CD4 testing, was transitioning to being used only as an indicator for advanced HIV illness.
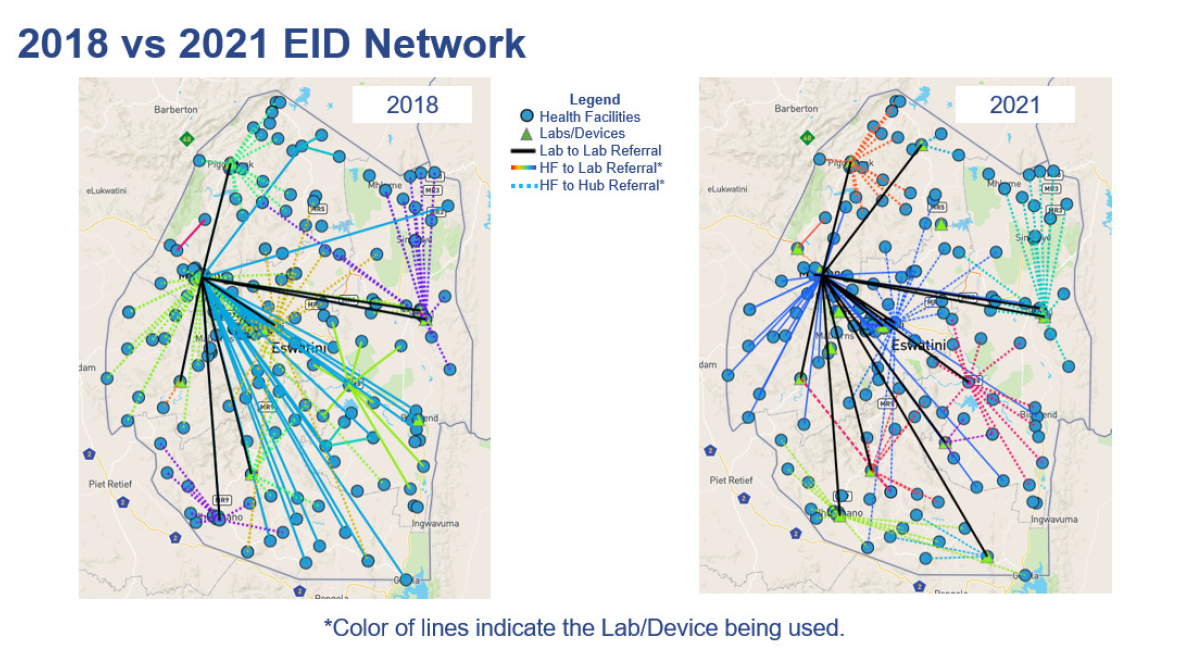
The country also introduced Early Infant Diagnosis (EID), placing one low-throughput EID machine at the National Reference Lab (NRL) to handle all testing for the country.
This new testing capacity was an important development for adults and infants who needed HIV testing in Eswatini. But the country still faced several challenges:
- Viral load testing capacity was not sufficient to meet testing targets
- EID was centralized, with a complex specimen referral network, hence had long turnaround times
- Instrument downtime was too high
- The CD4 network needed to be streamlined, with obsolete instruments removed